

After a car accident, we might find ourselves in an emergency room, dressed in an exam gown and covered by a thin blanket on a hospital gurney. In that moment we have no way to speed through a doctor’s evaluation, diagnostic testing, or clinical treatment. There’s no steering wheel to grab on to and no accelerator pedal on the bed. As the experience progresses, clinicians explain their findings and recommendations. A nurse comes with paperwork. Finally, return home is near. In the days to follow, an auto repair facility will address vehicle damage. But it may take weeks to feel better — physically and mentally — or not. Perhaps an outpatient chiropractic visit will become necessary, or a physical therapy treatment will be needed. What is certain is that soon medical bills will arrive. In the increasingly complex healthcare environment, casualty claims management makes a difference for individuals injured during a car accident. Through the combination of clinical expertise and technology, auto casualty solutions optimize the digital processing of medical bills causally related to motor vehicle collisions. While every accident is unique for the people, time, place and circumstances involved, accumulating data-driven insights show how macro-trends impact auto injury claims severity and challenge auto insurers.
Jurisdictional Trends
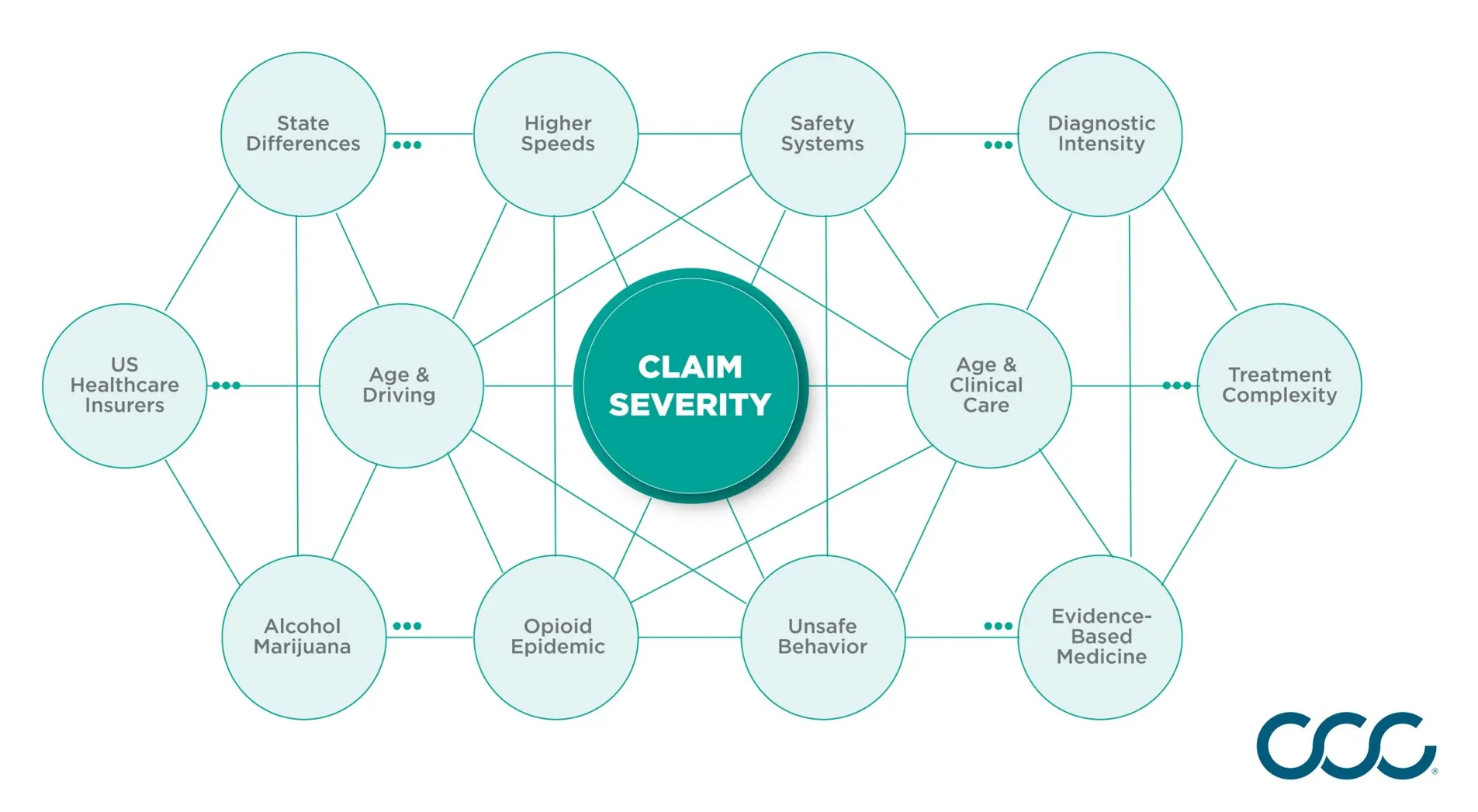
State jurisdictions differ in auto personal injury protection insurance regulations. However, recent data reveals less-apparent state-based influences on auto casualty claims risk. Regulations on speed limits, marijuana legalization, alcohol-associated driving, and the opioid epidemic vary significantly across the U.S., reshaping patterns of auto casualty claim severity. Road Speed Limits Over the last decade road speed limits have increased in many localities, including the states of Wisconsin, Illinois and Indiana. Across the U.S., the National Highway Transportation Safety Administration documented fewer single and multi-vehicle collisions occurring at less than 30 mph in police-reported crashes, with about 76% of all these crashes happening at 30 mph or greater. More than 86% of injury crashes were reported at 30 mph or greater. There is a known relationship between change in velocity, or Delta V, at collision impact and injury potential. Consequently, higher speed collisions can result in more trauma, surgeries and complications, as well as longer rehabilitation periods, thereby increasing casualty claims severity. Marijuana Legalization Impaired driving risk is non-uniform across the U.S. For example, states have varied in their actions on marijuana legalization. Currently, Alaska, Washington, Oregon, California, Nevada, Colorado, Michigan, Vermont, Massachusetts, Illinois and Maine have legalized consumer recreational and medical marijuana use, while 21 other states have authorized prescribed medical marijuana. In its 2019 report, the U.S. Congressional Research Services summarized the US National Academy of Sciences’ significant finding of statistical association between marijuana use and increased risk of motor vehicle accidents. Alcohol-Associated Impaired Driving Differences in state alcohol-associated impaired driving patterns have been noteworthy as well. As reported by the Department of Transportation’s National Center for Statistics and Analysis based on 2017 data, Texas, Wyoming and Montana had 35% or more alcohol-impaired driving fatalities, while Rhode Island’s experience was at 41%, Connecticut at 43% and Washington D.C. at 51%.Alcohol-impaired driving fatalities are an indicator of the prevalence of driving under the influence in the state of record, as coroner involvement and death certificate data are rigorously addressed. These fatalities have been understood as the “tip of the iceberg” when it comes to the scale of each state’s challenge to combat drunken driving behaviors. Opioid Associated Driving Fatalities Impaired driving attributable to use of opioids also intensified across the last decade. For the U.S., the percentage of fatally injured drivers who tested positive for prescription opioids rose seven-fold from 1% in 1995 to over 7% in 2015. According to the U.S. Centers for Disease Control and Prevention, between 2016 and 2017, Oregon, Arizona, Minnesota, and North Carolina experienced significantly increased numbers of opioid deaths, signaling epidemic crises in those areas. While public awareness has increased about the opioid use prevalence in every neighborhood and socioeconomic group, law enforcement and healthcare providers continue to struggle to meet the escalating epidemic’s fallout. There is little documented indication that the opioid epidemic has abated, suggesting continued driving risk associated with prescribed and illicit opioid use.
Aging Populations
A second macro trend shifting U.S. auto casualty claims severity is seen with the growth of aging U.S. populations. A key data insight is that the generational transition with the maturing of “Baby Boomers” has not been distributed evenly across all states. Between 2007 and 2016, the number of people aged 65 years or older in the United States increased by 30% (males by 35% and females by 26%), with the total population across all age groups increased by 7%. States most recently affected by this demographic shift include Texas, California, Florida, Georgia, North Carolina, Washington and Arizona. As generational aging has impacted state populations, the distribution of licensed drivers has trended older as well. For example, of Michigan’s 2017 population, 72.3% were reported as licensed drivers. In 2017, one out of five Michigan licensed drivers (20.5%) was aged 65 years or older. Of these, 3.4% were accountable for 50,807 of Michigan’s total number of 314,921 crashes, suggesting a highly disproportionate risk of collision for senior drivers. Substantiating the recognition of age-related driving risk for seniors, a published 2017 national report of age-related differences in fatal intersection crashes shows teens and drivers aged 55 years and older were “over-involved” in fatal intersection crashes, while drivers aged 20 to 54 years were “under-involved.” Remarkably, the study showed that the fatal intersection driving risk across all driver age groups was doubled by age 85.
Treatment Complexity
The third major trend related to auto casualty claims severity is greater treatment complexity. Treatment complexity in auto casualty reflects broader healthcare initiatives related to evidence-based medicine (EBM) guidelines, diagnostic intensity, and aging-related care considerations.
- EBM guidelines, protocols, and recommended practices influence clinical evaluation, treatment and rehabilitation nationally, by jurisdictional and on a specialty basis. As electronic medical record systems penetrate large health system operations, EBM’s incorporation into patient evaluation protocols, prescribing systems, diagnostic testing algorithms and care paths is more routine. For example, the consistent and expanded use of diagnostic imaging with suspected head injury or blunt abdominal trauma (BAT) has been in part due to generally accepted EBM guidelines.
- Attention to diagnoses commonly associated with motor vehicle accidents has increased. For example, heightened monitoring of traumatic brain injury diagnoses has evolved in many states in tandem with state emergency medical systems (EMS) and state trauma registries. As a result, there is wider awareness the association between motor vehicle accidents and the occurrence of clinical conditions such as headaches, concussion, and traumatic brain injury or TBI. First responders and emergency clinical providers are trained to evaluate for these conditions in auto accidents, just as today team coaches are expected to manage player risk of concussion in sports situations across all age groups.
- Age-related treatment complexity, for pediatric and senior populations, is now widely recognized. In this regard, the American College of Surgeons and the Pediatric Trauma Society’s guidelines have been influential, as these are the basis for EMS protocols in most states. Clinically relevant concerns include medical frailty; eligibility for certain types of care; or difficulty with post-injury rehabilitation protocols. Regarding seniors, data show that in injury treatment scenarios, older patients are likely to have more than one pre-existing medical condition, take multiple medications, and be at risk for complications even with simple procedures.
Summary
Jurisdictional differences, aging populations and increasing treatment complexity are impacting auto casualty risk and claims management. These trends are likely to continue into 2021 and beyond. The good news is that technology solutions can assist carriers in managing locational, generational and healthcare-related changes in auto casualty claims severity. Moreover, by aligning deep medical insights about how auto crashes might result in injuries, along with state-specific automated processing of healthcare transactions, medical bill payments can be addressed more efficiently. Efficiency gains rely on the use of artificial intelligence, machine learning, and data analytics to advance digital claims management. These three key innovations link the sciences of engineering and medicine. As a result, the time-in-process for resolving the reimbursed relationships in an auto casualty claim between providers, healthcare facilities, and allied health resources can be reduced. Furthermore, the insured can benefit from the knowledge that their insurer is addressing their claim with expert processing relying on the facts and details personal to their accident. With the right mix of expertise, comprehensive solutions, network management and technology, claims professionals can get to the right decision faster. Visit CCC’s Casualty Claims page to learn more and explore our available solutions.





